by Editor | Apr 5, 2016 | Health Care, Menopause, Perimenopause
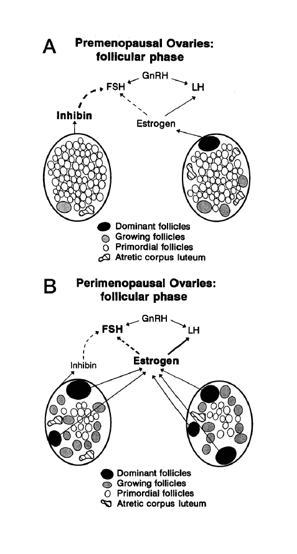
Making sense of the many names for women’s reproductive aging by Dr. Jerilynn C. Prior Jerilynn C. Prior BA, MD, FRCPC, ABIM, ABEM is a Professor of Endocrinology and Metabolism at the University of British Columbia in Vancouver, B.C. She is the founder (2002) and...
by David Linton | Dec 26, 2015 | Books, Humor, Media, Menopause
The holiday season brings plenty of opportunities to celebrate as well as to reflect on our lives, our society, and the state of the world. So, here’s an opportunity to reflect on the state of the menstrual ecology, a look back at a post from three years ago,...

by Chris Bobel | Jun 16, 2014 | Activism, Anatomy, Birth Control, Books, Celebrities, Coming off the pill, Communication, DIY, FemCare, Fertility, Girls, Health Care, History, Hormones, Humor, Language, Law/Legal, Media, Men, Menarche, Menopause, Menstruation, Meta, Motherhood, New Research, Objects, Ovulation, Pharmaceutical, Philosophy, PMS, Politics, Pregnancy, Religion/Spirituality, Reproduction, Sex, Sports, Theater, Toxic Shock Syndrome
…...
by Heather Dillaway | May 23, 2014 | Communication, Menopause, New Research, Perimenopause, Philosophy
A recent study by researchers at La Trobe University and Monash University in Melbourne, Australia, suggests that working women “need more managerial support [while] going through menopause.” This “Women at Work” study explored the health and wellbeing of working...
by Heather Dillaway | Nov 7, 2013 | Communication, Menopause, Perimenopause
I’ve been thinking a lot about the messages that women do or don’t get at menopause. Because of this, I decided to come up with a list of things that women would love to hear at menopause (or perimenopause, if we are talking about when women experience the...
