
by Elizabeth Kissling | Mar 20, 2013 | Girls, Health Care, Menstruation
You’re busy celebrating Women’s History Month, the Ides of March, Pi(e) Day, St. Patrick’s Day, not to mention Spring Break and numerous lesser known awareness days and months. But don’t let Endometriosis Awareness Month slip away....
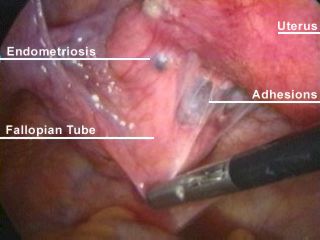
by Elizabeth Kissling | Dec 16, 2011 | Anatomy, Health Care
I’ve recently developed a whole new understanding of why it takes so long for women to receive a diagnosis of and treatment for endometriosis. It’s not just the constraints of menstrual etiquette or the belief that painful periods are normal, especially...
by Elizabeth Kissling | Nov 29, 2010 | Dysmenorrhea, Health Care, Menstruation, New Research
A cross-sectional study published in the November, 2010, issue of Fertility and Sterility reports that very painful menstrual periods during the teen years (that is, period pain so severe that girls miss school) may be predictive of an increased risk of developing...

by Elizabeth Kissling | Sep 10, 2010 | Dysmenorrhea, Girls, Menstruation, New Research
A new study published in the Journal of Pediatric Adolescent Gynecology reports on a study of how dysmenorrhea affects girls’ relationships with families and friends and school performance for girls in Turkey. Previously, we reported on research documenting that...
by Elizabeth Kissling | Jul 26, 2010 | Dysmenorrhea, Menstruation, New Research
Women have long been advised that exercise is among the best pain relievers for painful periods. But a new Cochrane Review (also published in July, 2010, issue of Obstetrics & Gynecology) indicates that research confirming that advice is inconclusive. Yet, the...
