by Elizabeth Kissling | Dec 13, 2010 | Advertising, Media, Menstruation, Pharmaceutical, Television
At least according to the newest ad for Kitadol, a menstrual pain reliever sold in Chile. According to The Viking Network, Viking women retained property and inheritance rights after marriage, plus the right to divorce a husband who mistreated her or their children,...

by Elizabeth Kissling | Sep 10, 2010 | Dysmenorrhea, Girls, Menstruation, New Research
A new study published in the Journal of Pediatric Adolescent Gynecology reports on a study of how dysmenorrhea affects girls’ relationships with families and friends and school performance for girls in Turkey. Previously, we reported on research documenting that...
by Elizabeth Kissling | Jul 26, 2010 | Dysmenorrhea, Menstruation, New Research
Women have long been advised that exercise is among the best pain relievers for painful periods. But a new Cochrane Review (also published in July, 2010, issue of Obstetrics & Gynecology) indicates that research confirming that advice is inconclusive. Yet, the...
by Elizabeth Kissling | Mar 24, 2010 | Dysmenorrhea, Language, Menstruation, New Research, Newspapers, Pharmaceutical
London newspaper The Telegraph reports on the development of a new medical treatment for dysmenorrhea, or painful periods. The article contains very little information about the new pill — most of the article describes the variety of misery some women experience...
by Elizabeth Kissling | Mar 11, 2010 | Anatomy, Dysmenorrhea, FemCare, Menarche, Menstruation, New Research
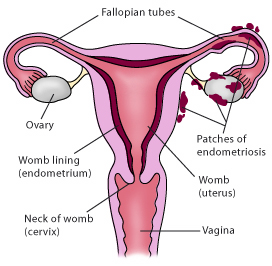
In a controlled study of 268 Australian women with surgically confirmed moderate-to-severe endometriosis (cases) and 244 women without endometriosis (controls), researchers found that characteristics of a woman’s early menstrual cycles were associated with later...
