by Chris Bobel | Mar 17, 2014 | Activism, Anatomy, Communication, Independent Film, Internet, Menstruation, Objects
Readers—I need your help! Next month, I will participate in a friendly debate at the Museum of Modern Art about Sputniko!’s provocative piece “Menstrutation Machine.” We’ve written about Menstruation Machine on re:Cycling before. In short, the metal device is equipped...

by Elizabeth Kissling | Mar 20, 2013 | Girls, Health Care, Menstruation
You’re busy celebrating Women’s History Month, the Ides of March, Pi(e) Day, St. Patrick’s Day, not to mention Spring Break and numerous lesser known awareness days and months. But don’t let Endometriosis Awareness Month slip away....
by Laura Wershler | Jan 20, 2012 | Birth Control, Communication, Dysmenorrhea, Health Care, Menstruation, New Research, Pharmaceutical
Is there a woman over the age of 18 anywhere who doesn’t know that taking the birth control pill can make her periods lighter and less painful? Most women know this, but not many know why. The news stories swirling around a new study about the pill and period pain...
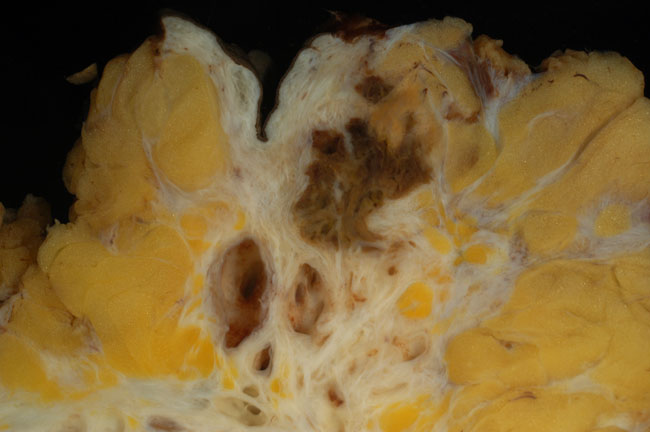
by Elizabeth Kissling | Dec 16, 2011 | Anatomy, Health Care
I’ve recently developed a whole new understanding of why it takes so long for women to receive a diagnosis of and treatment for endometriosis. It’s not just the constraints of menstrual etiquette or the belief that painful periods are normal, especially...

by Elizabeth Kissling | Feb 16, 2011 | Dysmenorrhea, Menstruation, New Research
A new study published in the Journal of Experimental Psychology reports that menstrual pain — like annoying noises and tedious computer tasks — hurts more in retrospect, if we anticipate experiencing it again: In the culminating field study of 180 women...
