by Editor | Apr 28, 2016 | Menopause, Perimenopause
Writing Menopause, a diverse literary collection about menopause to be published in the spring of 2017 by Inanna Publications, was first introduced to the Society for Menstrual Cycle Research in a session presented at our June 2015 biennial conference in Boston. The...
by Editor | Apr 26, 2016 | Books, Literature, Menopause, Perimenopause
Writing Menopause, a diverse literary collection about menopause to be published in the spring of 2017 by Inanna Publications, was first introduced to the Society for Menstrual Cycle Research in a session presented at our June 2015 biennial conference in Boston. The...
by Editor | Apr 5, 2016 | Health Care, Menopause, Perimenopause
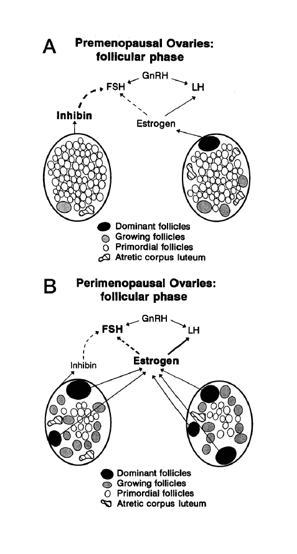
Making sense of the many names for women’s reproductive aging by Dr. Jerilynn C. Prior Jerilynn C. Prior BA, MD, FRCPC, ABIM, ABEM is a Professor of Endocrinology and Metabolism at the University of British Columbia in Vancouver, B.C. She is the founder (2002) and...
by David Linton | Dec 26, 2015 | Books, Humor, Media, Menopause
The holiday season brings plenty of opportunities to celebrate as well as to reflect on our lives, our society, and the state of the world. So, here’s an opportunity to reflect on the state of the menstrual ecology, a look back at a post from three years ago,...
by Editor | Jun 17, 2015 | Health Care, Hormones, Literature, Menopause, Menstruation, New Research, Pharmaceutical
Free access to Women’s Reproductive Health, the journal launched by the Society for Menstrual Cycle Research in 2014, is available to all SMCR members. To become a member of the society or to obtain a subscription contact info@menstruationresearch.org. For...
