by Holly Grigg-Spall | Jun 4, 2013 | Activism, Birth Control, Girls, Health Care, Hormones, Menstruation
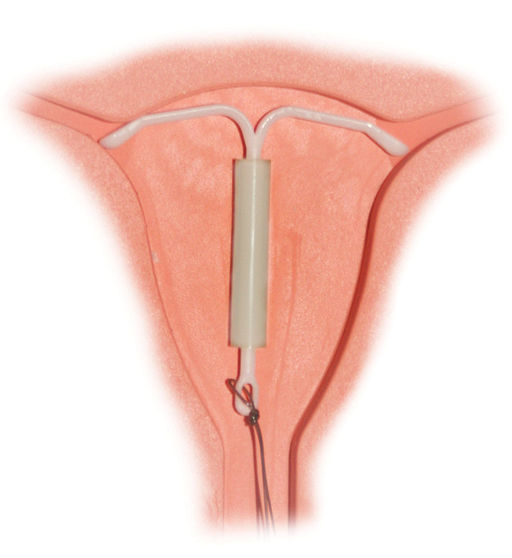
Do women using the Mirena hormonal IUD have their period? Does it suppress the hormone cycle for all women or just some? How does it work to prevent pregnancy exactly? It seems these questions can’t be answered even by the assumed experts. We are told the Mirena...

by Kati Bicknell | Nov 1, 2012 | Birth Control
Who among us wants to invite a T-shaped piece of plastic or metal to live in our uterus for the next 5 to 10 years, just for fun? No one! But if it’s to prevent pregnancy that’s a different story. IUDs may be uncomfortable and annoying but women still use them because...
by Elizabeth Kissling | Jul 8, 2010 | Birth Control, Dysmenorrhea, Girls, Health Care, Menorrhagia, New Research, Pharmaceutical
A new study published in the Journal of Obstetrics and Gynecology has found that adolescents are usually able to tolerate the Mirena® IUD rather well. The mean age of girls in this British study was 15.3 years, and they were prescribed the Mirena® for painful and/or...
by Chris Hitchcock | Apr 20, 2010 | Birth Control, Health Care, Menstruation, Ovulation, Pharmaceutical, Reproduction, Sex
It’s starting. With the approaching 50th anniversary of the birth control pill, there will be a flood of anniversary celebrations and reviews of birth control methods. Which is good. We should have those discussions more often. Just say “no” (on the...
by Elizabeth Kissling | Feb 9, 2010 | Advertising, Birth Control, Law/Legal, Pharmaceutical
Guest Post from Evil Slutopia There are Tupperware parties, Passion Parties, Pampered Chef parties, and…Mirena IUD parties? Yes, apparently these events popped up early last year and were a joint effort from Bayer Pharmaceuticals and the mom marketing site Mom...
