by Editor | Jun 17, 2015 | Health Care, Hormones, Literature, Menopause, Menstruation, New Research, Pharmaceutical
Free access to Women’s Reproductive Health, the journal launched by the Society for Menstrual Cycle Research in 2014, is available to all SMCR members. To become a member of the society or to obtain a subscription contact info@menstruationresearch.org. For...
by Laura Wershler | Mar 27, 2015 | Literature, Menstruation, Ovulation, Reproduction
In Parts 1 and 2, I wondered why author Ann Patchett chose not to include information about menstruation, femcare products and birth control that, logically, would have enhanced her novel’s inciting premise—lifelong menstruation and fertility—while retaining the...
by Laura Wershler | Aug 28, 2014 | Birth Control, Coming off the pill, Hormones
re-blogging re:Cycling In celebration of our fifth anniversary, we are republishing some of our favorite posts. This post by Laura Wershler originally appeared April 4, 2012, and has received nearly 600 comments. To avoid confusion, we have closed comments on this...
by Paula Derry | Oct 14, 2013 | Hormones, Menopause, Menstruation
The North American Menopause Society held its annual meeting Oct. 9 to 12. An article posted a few days earlier stated that hot flashes would be “extensively discussed” at the meeting because “temperature control is such a preoccupation for menopause.” There would be...
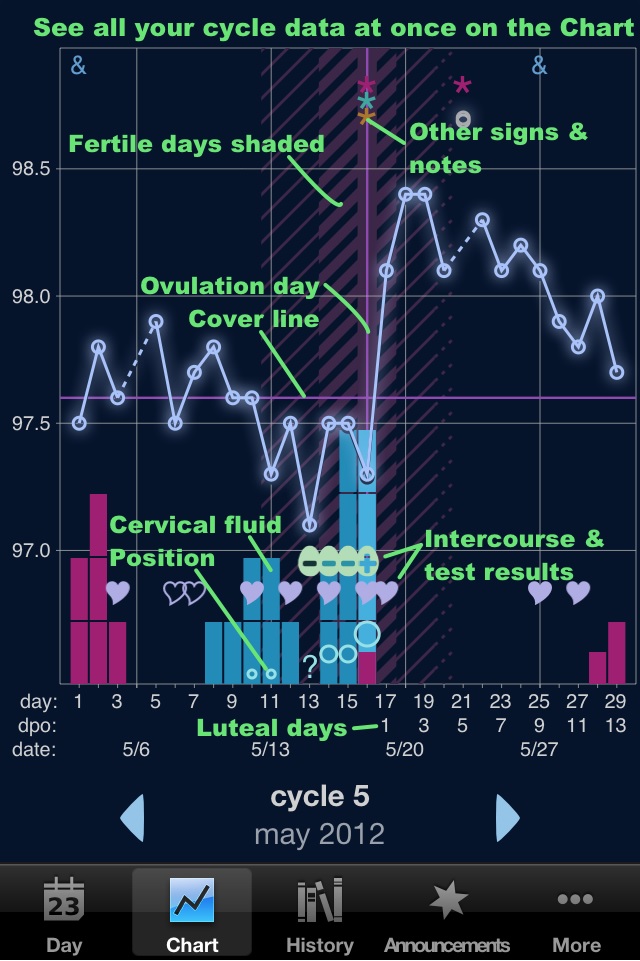
by Chris Bobel | Sep 2, 2013 | Anatomy, Birth Control, Fertility, Health Care, Menstruation, Ovulation, Reproduction
Guest Post by Amy Sedgwick, HRHP, Red Tent Sisters While there are no shortage of apps designed to help women track their periods, finding an app that meets the needs of women who are practicing fertility awareness methods (FAM) for birth control or conception can be...
