by Laura Wershler | Aug 28, 2014 | Birth Control, Coming off the pill, Hormones
re-blogging re:Cycling In celebration of our fifth anniversary, we are republishing some of our favorite posts. This post by Laura Wershler originally appeared April 4, 2012, and has received nearly 600 comments. To avoid confusion, we have closed comments on this...
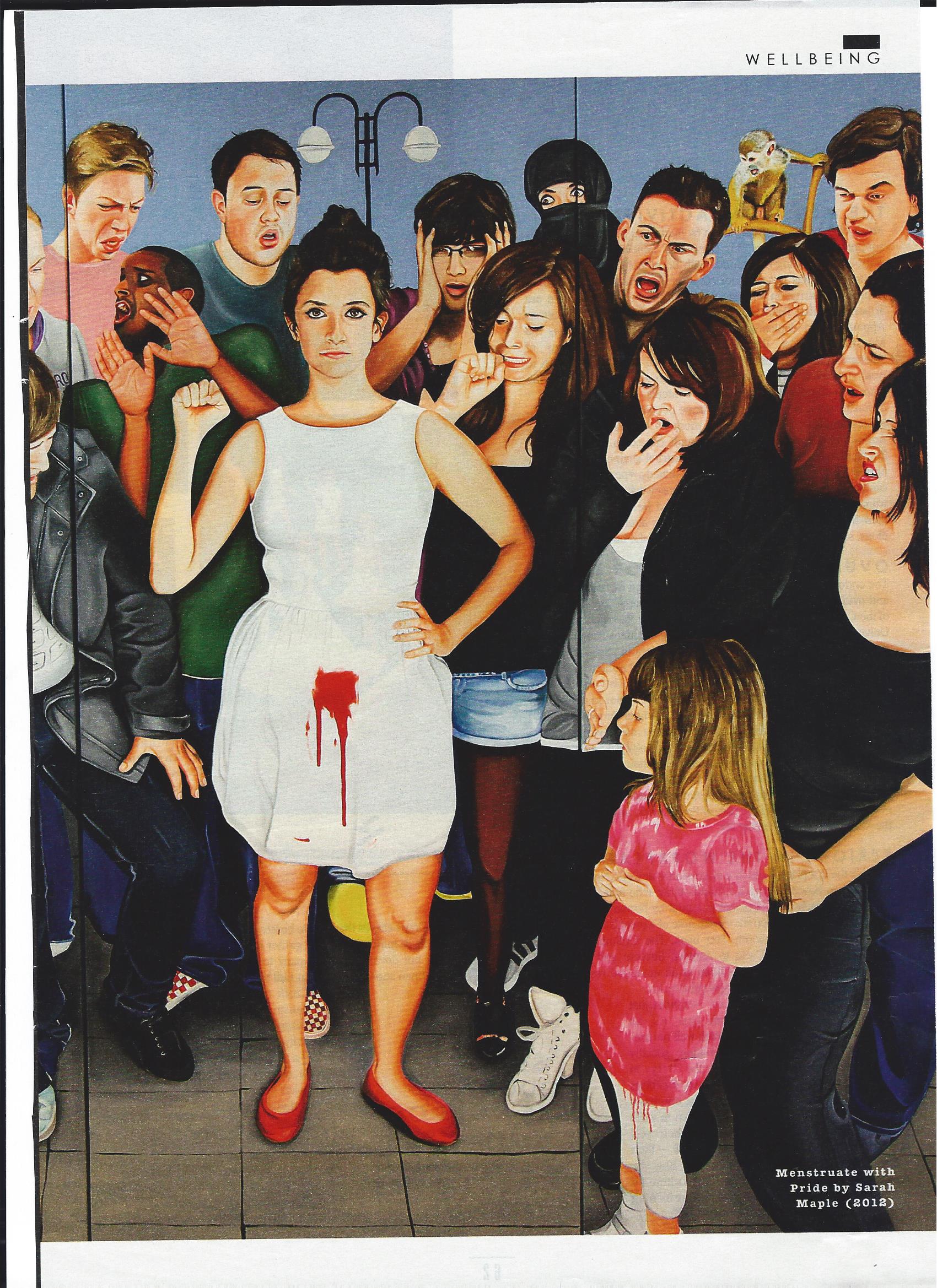
by Holly Grigg-Spall | Nov 19, 2013 | Activism, Birth Control, Books, Disposable menstrual products, FemCare, Humor, magazines, Media, Menstruation, Newspapers, Ovulation, Pharmaceutical, Reusable menstrual products
Recently I was fortunate enough to be asked to lend an excerpt of my recently released book to the UK Sunday Times Style magazine. The mostly fashion-centric Style magazine is not really known for its edginess or risk-taking (except perhaps in the realm of shoe and...
by Elizabeth Kissling | Sep 13, 2013 | Birth Control, Books, Coming off the pill
It’s been more than 20 years since Susan Faludi first published Backlash (with the provocative subtitle, The Undeclared War Against American Women), her thorough documentation of the ways women and feminism were under attack in the U.S. The War Against Women has...
by Holly Grigg-Spall | Aug 26, 2013 | Activism, Advertising, Birth Control, Coming off the pill, Health Care, History, Hormones, Media, Men, Menstruation, Pharmaceutical, PMS
My forthcoming book ‘Sweetening the Pill or How We Got Hooked on Hormonal Birth Control’ began to take shape on the pages of this blog and much of the process of its development was spurred on by the work of members of SMCR. As such, it seems only fitting,...
by Elizabeth Kissling | Sep 5, 2012 | Birth Control, Coming off the pill, Hormones, Pharmaceutical
Guest Post by Leslie Carol Botha Women’s Health Freedom Coalition Coordinator, Natural Solutions Foundation I still remember the first Society for Menstrual Cycle Research Conference I attended in Tucson, AZ in June, 1999. The statement that made the most impact...
