by Paula Derry | Nov 12, 2012 | Hormones, Menopause
I have two pretty contradictory sets of opinions about hot flashes. In a previous blog post, I emphasized one of them. Namely, that flashes are a mind/body phenomenon in which a woman’s interpretation of her physical experiences are central to her being distressed or...
by Elizabeth Kissling | Sep 5, 2012 | Birth Control, Coming off the pill, Hormones, Pharmaceutical
Guest Post by Leslie Carol Botha Women’s Health Freedom Coalition Coordinator, Natural Solutions Foundation I still remember the first Society for Menstrual Cycle Research Conference I attended in Tucson, AZ in June, 1999. The statement that made the most impact...
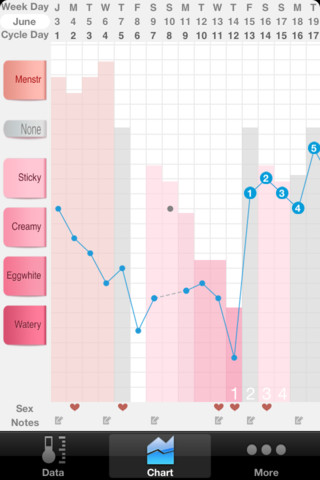
by Kati Bicknell | Aug 29, 2012 | Fertility, Menstruation, Ovulation
The Quantified Self is the idea that by tracking things about your body you can live a happier and healthier life. Hardware devices like the Fitbit and Withings scale measure your daily activity and weight respectively so people can set and reach activity and weight...
by Elizabeth Kissling | Aug 8, 2012 | Hormones, Pharmaceutical
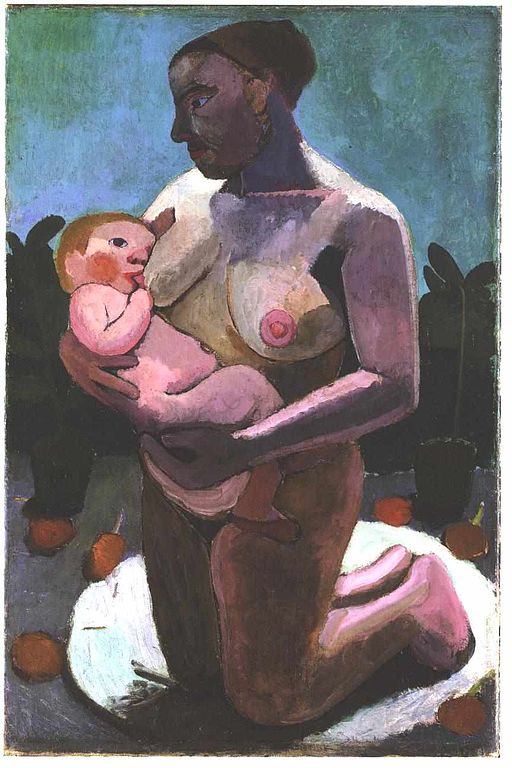
Let me say up front that I have limited direct experience with adoption. Some members of my extended family have adopted children, another has given up an infant for adoption, and I have friends who have adopted children, and other friends who are adopted. It was one...
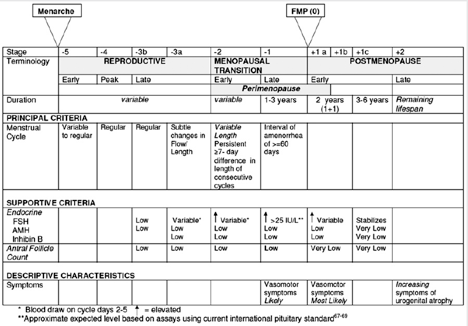
by Elizabeth Kissling | May 17, 2012 | Hormones, Language, Menopause, Menstruation, New Research
Guest Post by Jerilynn Prior, M.D. — Centre for Menstrual Cycle and Ovulation Research By “midlife muddle” I don’t mean the trouble concentrating or remembering names that sometimes occurs for all of us (but more frequently if we’ve wakened with night sweats and...
