by Laura Wershler | Jan 20, 2012 | Birth Control, Communication, Dysmenorrhea, Health Care, Menstruation, New Research, Pharmaceutical
Is there a woman over the age of 18 anywhere who doesn’t know that taking the birth control pill can make her periods lighter and less painful? Most women know this, but not many know why. The news stories swirling around a new study about the pill and period pain...
by Elizabeth Kissling | Nov 29, 2010 | Dysmenorrhea, Health Care, Menstruation, New Research
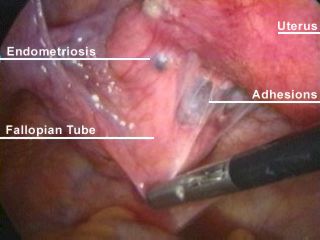
A cross-sectional study published in the November, 2010, issue of Fertility and Sterility reports that very painful menstrual periods during the teen years (that is, period pain so severe that girls miss school) may be predictive of an increased risk of developing...

by Elizabeth Kissling | Sep 10, 2010 | Dysmenorrhea, Girls, Menstruation, New Research
A new study published in the Journal of Pediatric Adolescent Gynecology reports on a study of how dysmenorrhea affects girls’ relationships with families and friends and school performance for girls in Turkey. Previously, we reported on research documenting that...
by Elizabeth Kissling | Jul 26, 2010 | Dysmenorrhea, Menstruation, New Research
Women have long been advised that exercise is among the best pain relievers for painful periods. But a new Cochrane Review (also published in July, 2010, issue of Obstetrics & Gynecology) indicates that research confirming that advice is inconclusive. Yet, the...
by Elizabeth Kissling | Mar 24, 2010 | Dysmenorrhea, Language, Menstruation, New Research, Newspapers, Pharmaceutical
London newspaper The Telegraph reports on the development of a new medical treatment for dysmenorrhea, or painful periods. The article contains very little information about the new pill — most of the article describes the variety of misery some women experience...
