by David Linton | Jan 15, 2014 | Books, Film, Media, Men, Menstruation
In 1967, the same year as the previously discussed Diary of a Mad Housewife, Ira Levin’s Rosemary’s Baby was published and eventually climbed to Number Seven on the Best Seller list for that year. It then went on to become a successful feature film in 1968...
by David Linton | Jan 8, 2014 | Books, Film, Media, Men, Menstruation
In 1967 a new novel, Diary of a Mad Housewife by Sue Kaufman, struck a chord with Boomer Generation women, the post-war era’s cohort who were already the subject of Betty Friedan’s 1963 The Feminine Mystique and who are characterized today in...

by Elizabeth Kissling | Mar 20, 2013 | Girls, Health Care, Menstruation
You’re busy celebrating Women’s History Month, the Ides of March, Pi(e) Day, St. Patrick’s Day, not to mention Spring Break and numerous lesser known awareness days and months. But don’t let Endometriosis Awareness Month slip away....
by Elizabeth Kissling | May 17, 2012 | Hormones, Language, Menopause, Menstruation, New Research
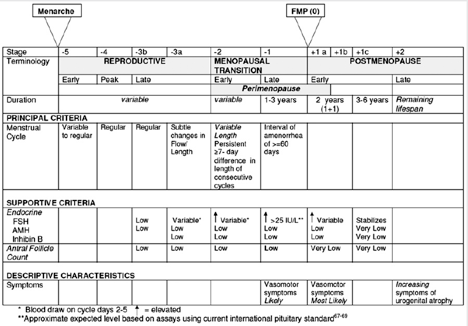
Guest Post by Jerilynn Prior, M.D. — Centre for Menstrual Cycle and Ovulation Research By “midlife muddle” I don’t mean the trouble concentrating or remembering names that sometimes occurs for all of us (but more frequently if we’ve wakened with night sweats and...
by Elizabeth Kissling | Jan 20, 2010 | Dysmenorrhea, Menstruation, New Research, Pharmaceutical
A new meta-analysis of previous research on acetaminophen (also known as paracetamol outside the U.S.) vs. NSAIDs (nonsteroidal anti-inflammatory drugs) for treatment of menstrual pain indicates that NSAIDs are more effective. NSAIDs include aspirin, ibuprofen, and...
