
by Holly Grigg-Spall | Apr 8, 2014 | Amenorrhea, Birth Control, Celebrities, Coming off the pill, Communication, Disposable menstrual products, FemCare, Health Care, Menarche, Menstruation, Pharmaceutical, Politics, Reusable menstrual products
A few weeks back I did an interview with Leslie Botha regarding the distribution of Depo Provera to women in developing countries. Recently Leslie shared with me an email she received from someone working in a family planning clinic in Karnataka, India. He described...
by Holly Grigg-Spall | Mar 11, 2014 | Birth Control, Books, Health Care, Menstruation, Ovulation, Pharmaceutical
I’d given up reading the comments on online articles for the good of my mental health when a small slip last week steeled my resolve. In response to an article exploring the arguments made by “birth control truthers” a concerned father decided to have his say, taking...

by Chris Bobel | Nov 26, 2013 | Activism, Birth Control, Books, Celebrities, Coming off the pill, Communication, Disposable menstrual products, DIY, FemCare, Film, Independent Film, Literature, Men, Menstruation, Pharmaceutical, Reusable menstrual products
The recent death of writer Doris Lessing led me to revisit her work a bit. * Author of more than 50 books as well as an opera, Lessing was brave. She spanned genres, refused to tow a singular ideological line and used her Nobel Prize moment to remind us that privilege...
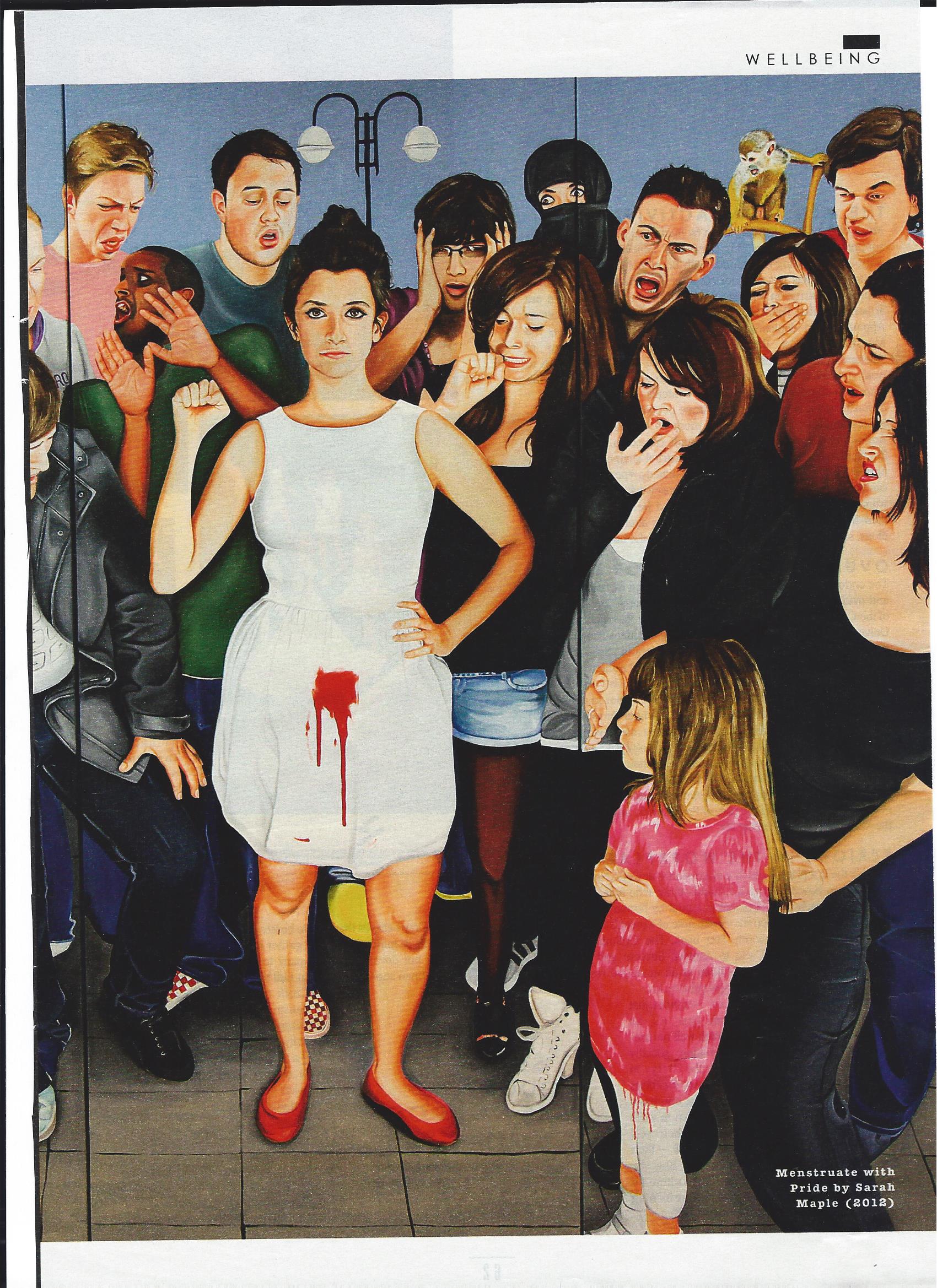
by Holly Grigg-Spall | Nov 19, 2013 | Activism, Birth Control, Books, Disposable menstrual products, FemCare, Humor, magazines, Media, Menstruation, Newspapers, Ovulation, Pharmaceutical, Reusable menstrual products
Recently I was fortunate enough to be asked to lend an excerpt of my recently released book to the UK Sunday Times Style magazine. The mostly fashion-centric Style magazine is not really known for its edginess or risk-taking (except perhaps in the realm of shoe and...
by Laura Wershler | Oct 16, 2013 | Activism, Birth Control, Books, Coming off the pill, Health Care, Hormones, Menstruation, Ovulation, Pharmaceutical
I had the privilege of writing the foreword for Holly Grigg-Spall’s recently published book Sweetening the Pill: Or How We Got Hooked on Hormonal Birth Control. It’s astounding to me that more than 30 years ago, before Holly was born, I was asking some of...
by Holly Grigg-Spall | Aug 26, 2013 | Activism, Advertising, Birth Control, Coming off the pill, Health Care, History, Hormones, Media, Men, Menstruation, Pharmaceutical, PMS
My forthcoming book ‘Sweetening the Pill or How We Got Hooked on Hormonal Birth Control’ began to take shape on the pages of this blog and much of the process of its development was spurred on by the work of members of SMCR. As such, it seems only fitting,...
Page 2 of 16«12345...10...»Last »
