
by Laura Wershler | Sep 8, 2015 | Girls, Menarche, Menorrhagia
Guest Post by Dr. Lara Briden, ND The onset of menstruation (menarche) is an important time for girls. It heralds their future fertility, of course, but it’s much more than that. Menarche is also when girls start to make female hormones for the first time. Making...
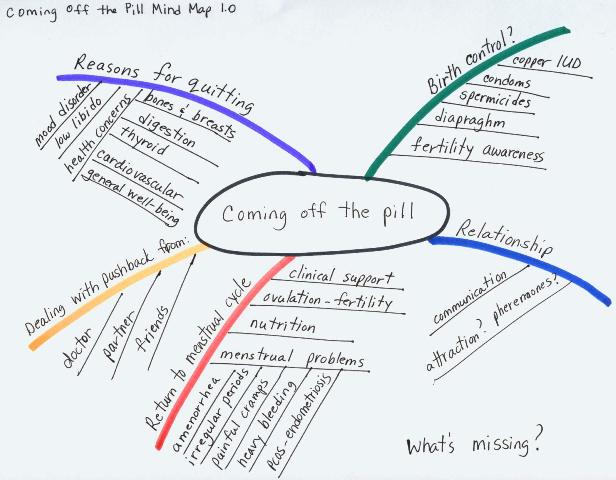
by Laura Wershler | Mar 7, 2012 | Activism, Amenorrhea, Birth Control, Coming off the pill, Communication, Dysmenorrhea, Health Care, Hormones, Menorrhagia, Menstruation, Ovulation, Pharmaceutical, PMS, Reproduction
Everybody can use a good map to help them get to where they’re going. Why not women heading to the land of non-hormonal contraception? In my post on January 11, 2012 I asked if coming off the pill was a growing trend. I proposed to write a series of posts about...
by David Linton | Sep 1, 2011 | Film, Independent Film, Literature, Men, Menorrhagia, Menstruation, Sex
The taboos against menstrual sex are ancient and deep-seated. Despite the well established fact that sexual intercourse during the period is not medically counter-indicated nor somehow debilitating to women and, furthermore, that some women find the experience more...
by Elizabeth Kissling | Jan 24, 2011 | Advertising, Media, Menorrhagia, Menstruation, Pharmaceutical, Television
The US Food and Drug Administration (FDA) approved tranexamic acid tablets as treatment for heavy menstrual bleeding more than a year ago, but you probably haven’t seen much of this television commercial to promote the drug (brand name Lysteda). Matthew Arnold...
by Elizabeth Kissling | Oct 11, 2010 | Menorrhagia, Menstruation, New Research, Pharmaceutical
Nearly a year ago, we shared news of FDA approval of tranexamic acid tablets as treatment for heavy menstrual bleeding. Today we learned of successful clinical trials of the drug this purpose: The current issue of Obstetrics & Gynecology includes the results of a...
by Elizabeth Kissling | Jul 8, 2010 | Birth Control, Dysmenorrhea, Girls, Health Care, Menorrhagia, New Research, Pharmaceutical
A new study published in the Journal of Obstetrics and Gynecology has found that adolescents are usually able to tolerate the Mirena® IUD rather well. The mean age of girls in this British study was 15.3 years, and they were prescribed the Mirena® for painful and/or...
