by Elizabeth Kissling | Jul 8, 2010 | Birth Control, Dysmenorrhea, Girls, Health Care, Menorrhagia, New Research, Pharmaceutical
A new study published in the Journal of Obstetrics and Gynecology has found that adolescents are usually able to tolerate the Mirena® IUD rather well. The mean age of girls in this British study was 15.3 years, and they were prescribed the Mirena® for painful and/or...
by Elizabeth Kissling | Apr 28, 2010 | Dysmenorrhea, New Research, PMS
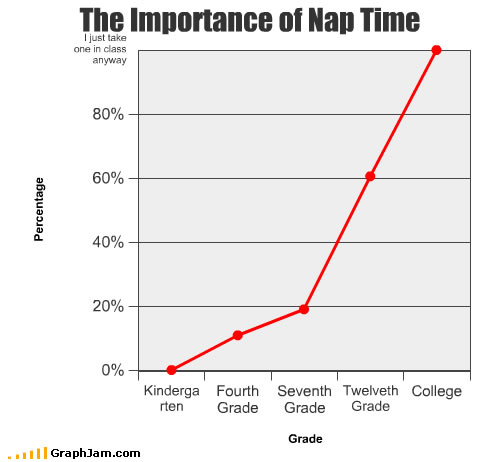
This is a very small study, but I don’t need much encouragement for an afternoon nap. Researchers wanted to test whether a mid-afternoon nap during the late-luteal phase of the menstrual cycle (commonly known as the premenstrual period) would improve symptoms of...
by Elizabeth Kissling | Mar 24, 2010 | Dysmenorrhea, Language, Menstruation, New Research, Newspapers, Pharmaceutical
London newspaper The Telegraph reports on the development of a new medical treatment for dysmenorrhea, or painful periods. The article contains very little information about the new pill — most of the article describes the variety of misery some women experience...
by Giovanna Chesler | Mar 12, 2010 | Amenorrhea, Dysmenorrhea, Film, Health Care, Independent Film, Menarche, Menstruation
(This post also published at the blog g6pix.) I’ll try not to sound too fan-girlish here as I write about the documentary Scrambled: A Journey through PCOS by Randi Cecchine, but admittedly, it is a difficult task. For in this film, which chronicles Cecchine’s...
by Elizabeth Kissling | Mar 11, 2010 | Anatomy, Dysmenorrhea, FemCare, Menarche, Menstruation, New Research
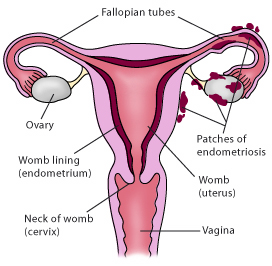
In a controlled study of 268 Australian women with surgically confirmed moderate-to-severe endometriosis (cases) and 244 women without endometriosis (controls), researchers found that characteristics of a woman’s early menstrual cycles were associated with later...
by Elizabeth Kissling | Jan 20, 2010 | Dysmenorrhea, Menstruation, New Research, Pharmaceutical
A new meta-analysis of previous research on acetaminophen (also known as paracetamol outside the U.S.) vs. NSAIDs (nonsteroidal anti-inflammatory drugs) for treatment of menstrual pain indicates that NSAIDs are more effective. NSAIDs include aspirin, ibuprofen, and...
