by David Linton | Feb 9, 2017 | Film, Newspapers, Television
Caitlin Moran is a prize-winning columnist for The Times of London where she has been publishing witty, pithy, and sometimes acerbic pieces about film, pop culture, politics and whatever random subject strikes her interest for the last 24 years. Unlike most regular...
by Laura Wershler | Mar 5, 2016 | Endometriosis, Internet, Media, Newspapers
Worldwide, and here at re:Cycling, March is #EndometriosisAwarenessMonth. To increase your knowledge of this insidious disease, read through this series of articles and personal stories, briefly quoted here, that were published by The Guardian last September. ...

by David Linton | Feb 16, 2016 | FemCare, magazines, Media, Newspapers, Television
It seems we’ve reached a tipping point, as Malcolm Gladwell would put it, or perhaps a paradigm shift, as Thomas Kuhn might say, in the level of acceptance of menstrual cycle references in mainstream media. As re:Cycling demonstrated recently in the time line of...
by David Linton | Dec 10, 2015 | Law/Legal, Media, Men, Newspapers
Much has been made of Donald Trump’s snarky remark about how the journalist Megan Kelly spoke to him at the Republican candidates’ debate on Aug. 6, 2015. And the news is dominated by stories about how social media are reshaping every aspect of our lives,...
by Heather Dillaway | Jan 31, 2014 | Celebrities, Communication, Hormones, Language, Media, Men, Menopause, Menstruation, Newspapers
According to a recent piece in The Times, a reputable English newspaper, symptoms are demeaning AND feminine. More specifically, the article reports on the prostate cancer experiences of Sir Michael Parkinson, or “Parky,” a famous British talkshow host. Parkinson...
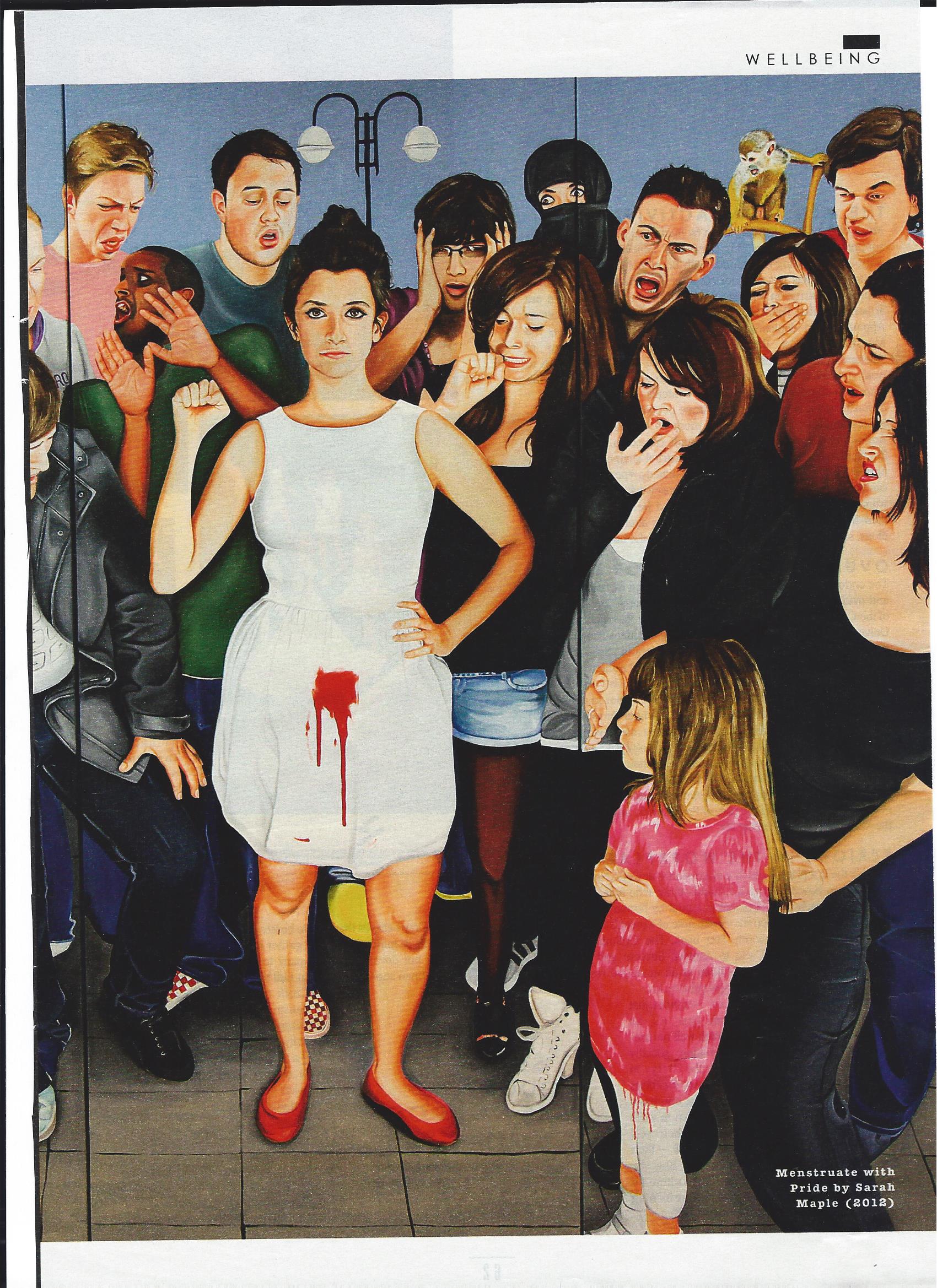
by Holly Grigg-Spall | Nov 19, 2013 | Activism, Birth Control, Books, Disposable menstrual products, FemCare, Humor, magazines, Media, Menstruation, Newspapers, Ovulation, Pharmaceutical, Reusable menstrual products
Recently I was fortunate enough to be asked to lend an excerpt of my recently released book to the UK Sunday Times Style magazine. The mostly fashion-centric Style magazine is not really known for its edginess or risk-taking (except perhaps in the realm of shoe and...
