
by Editor | Mar 14, 2017 | Endometriosis, Health Care, Sex
Guest Post by Dr. Sallie Sarrel, PT, ATC, DPT NOTE: This post was originally published on this blog on March 17, 2016. “We have emerged from the days of Freud and finger pointing that sexual pain is only psychological. Especially in the case of women with...
by Editor | Apr 5, 2016 | Health Care, Menopause, Perimenopause
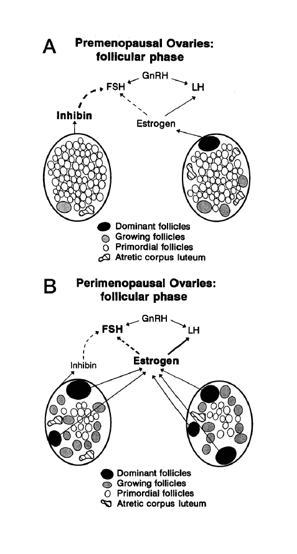
Making sense of the many names for women’s reproductive aging by Dr. Jerilynn C. Prior Jerilynn C. Prior BA, MD, FRCPC, ABIM, ABEM is a Professor of Endocrinology and Metabolism at the University of British Columbia in Vancouver, B.C. She is the founder (2002) and...
by Laura Wershler | Mar 31, 2016 | Endometriosis, Film, Health Care
The facts are eye-opening, the experts are compelling, but it is the voices of women talking about their lived experience with endometriosis that have the biggest impact in Endo What?, the documentary about the disease that premiered in New York City on March 16,...
by Editor | Mar 23, 2016 | Endometriosis, Health Care, Media
“…there are fewer than 100 surgeons in North America who have been identified as doing effective surgery for endometriosis.” Guest Post by Philippa Bridge-Cook, PhD Endometriosis has had more press attention in the last several weeks than it has had...
by Editor | Mar 17, 2016 | Endometriosis, Health Care, Sex
“We have emerged from the days of Freud and finger pointing that sexual pain is only psychological. Especially in the case of women with endometriosis, sexual pain is driven by physiologic reasons.” Guest Post by Dr. Sallie Sarrel, PT ATC DPT Sexuality is...

by Editor | Mar 15, 2016 | Endometriosis, Health Care, Sex
“Societal bias often tells us pain is simply ‘part of life’ and that symptoms of endometriosis like dyspareunia (painful sex) are somehow ‘normal’ or that we ‘shouldn’t talk about them.’ This is wrong.” Guest Post by...
